
Health Education flyers
UX research case study
Health education needs to be literacy-level appropriate for diverse
audiences to understand and act upon.
Project details
My role: Lead researcher (worked with project lead)
Type of Design: Printed flyers and digital to circulate online
Duration: 2 weeks
Tools: Zoom, Excel for analysis
Methods: User Interviews
Navigate to the sections or scroll for the process
The Problem
Majority of the refugees and immigrants in Clarkston, GA, speak a foreign language as their primary language in their households. English proficiency and low health literacy are barriers to accessing clinical services and delay preventive care which can lead to poor health outcomes.
Patients experience frustration when they cannot act upon health information given to them if they do not understand it.
Research goals
To understand and prioritize health messaging for a community with varying degrees of health literacy and English proficiency.
What are the most effective dissemination modalities for health messaging among Clarkston residents?
Interviews
I conducted 15 user interviews with community residents. My outreach was with community leaders who helped us recruit participants. Midway through the process, we couldn’t interview a second round of testing with participants so I gleaned off previous research and complemented with secondary research to inform the health messages.
We spoke to participants who were Clarkston residents, adults 18+ and aimed to speak to those with varying degrees of English proficiency.
Sample of interview questions:
1) In your own words, what do you think this flyer is about?
2) What do you think is the most important message on the flyer?
3) Who do you think this material is designed for?
4) Where might you imagine seeing this information?
5) Would you prefer to hear about this information from word of mouth, text, social media or flyer? Tell me more why you prefer that method.
6) From this flyer, do you think our goals are accomplished? Why or why not?
7) What changes could be made to help accomplish this goal, if any?
8) Do you think you could do what this material is suggesting? Why or why not?
9) Do you have any other recommendations we should include to improve this flyer? Y/N. What would that be?
Findings and recommendations
Below are the findings and recommendations I learned from our interviews. I used thematic analysis in Excel to analyze the qualitative data.
Findings
No. 1 - Translated messages
To improve our messaging, users suggested translating our messages to targeted audiences spoken in Clarkston to be more effective.
No. 2 - Social media is the preferred modality to distribute messages.
Facebook was specifically cited as people’s online avenue with some quotes stating, “It’s a digital world”, “Always on Facebook”, “Today’s issues are published in social media”. Our participants represent a global audience who are used to communicating to their families on social media.
No. 3 - Costs were the main reason for people to go see the clinic.
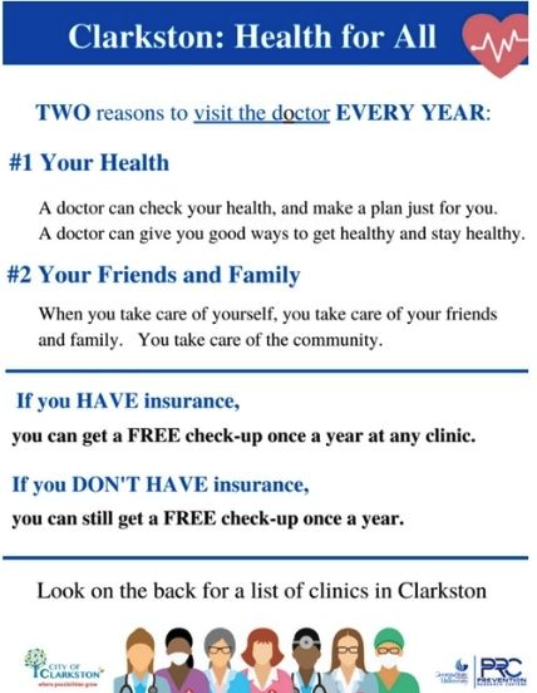
Having free services can be a strong determinant to motivate people to go to the clinic as it reduces the barrier for those who are un/underinsured (which was the community we were working in). The flyer shows actionable information, such as the specific clinics people can see based on their insurance status (no insurance or sliding scale), their addresses, have language using “free check-up”.
This explicit information raises awareness for those who were unaware of these services available for them.
Recommendations
Work with community members whom we have partnerships with to help translate these messages into the target languages spoken in Clarkston.
Include audio versions as well for those who may not be able to read in their language.
Create a pipeline of community members and leaders who are active on social media (especially on Facebook) to be able to share these health messages to their respective communities.
Share our organization facebook account on local signage and encourage people to follow us so people can have access to these health messages and news.
Include words that state “free services” or “free check-up” followed by actionable information in our health messages as these help encourage people to go to the clinic since we know costs are huge barriers to accessing healthcare.
Final design
This was the final flyer my colleagued designed for printed and digital flyers with clinic information on the back. The finding and recommendations contributed to future projects that we could glean essentially serving as a health education toolkit.
Challenges and Reflections
The challenging part of my project was recruiting participants from varying degrees of English proficiency to ensure we were designing for all levels. We only spoke to predominantly English speakers which led to self-selection bias as they most likely could read and understand our recruitment messages. Due to constraints around time, we weren’t able to translate our recruitment messages or interview guides to be included in our Institutional Review Board (IRB) since we needed the project to be completed in 2 weeks. The IRB reviews, approves or reject research projects involving conducting research with humans to ensure they’re done ethically.
We also planned on doing another round of interviews of iterations, but we didn’t have time so I had to glean from previous studies of best practices and from the literature on best practices to designing health messages for diverse communities similar to ours.